BONE LOSS IS FASTER THAN THE GAIN
*PREVENTABLE – (YES) *TREATABLE – (YES)
Goals: From NOF National Osteoporosis Foundation*

- Greater awareness about the importance of bone health, its impact on patients and caregivers, and cost-effective steps that can be taken to optimize bone health, prevent fractures and improve health outcomes.
- End the stigma and ageism associated with osteoporosis to assure that bone health gets the high priority and attention it deserves.
- Everyone deserves access to affordable, high-quality, age-appropriate bone health screening.
- Access to effective therapies to treat osteoporosis should be affordable and determined by each patient and their health professional.
- Best practices in care management and coordination for those who have suffered bone fractures should be replicated and appropriately incentivized.
KNOWN FACTS
ABOUT OSTEOPOROSIS
Osteoporosis is a disease of the bone.
• Osteoporosis is a “silent disease” until it is complicated by fractures, because you cannot feel your bones getting weaker, lighter and porous.
Osteoporosis is common.
INCIDENCE
Statistics from the International Osteoporosis Foundation, worldwide, 1 in 3 women over the age of 50 years and 1 in 5 men will experience osteoporotic fractures in their lifetime.
• Approximately 10 million Americans have osteoporosis and another 44 million have low bone density, living with increased risk.
• This means that half of all adults age 50 and older are at risk of breaking a bone and should be concerned about bone health.
• The disease is responsible for an estimated two million broken bones per year, yet nearly 80 percent of older Americans who suffer bone breaks are not tested or treated for osteoporosis.
• One in two women and up to one in four men over age 50 will break a bone due to osteoporosis.
• People with osteoporosis can break a bone from a minor fall, or in serious cases, even from simple actions like sneezing or bumping into furniture.
Osteoporosis is serious, even deadly.
• A woman’s risk of fracture is equal to her combined risk of breast, uterine and ovarian cancer.
• A man is more likely to break a bone due to osteoporosis than he is to get prostate cancer.
• 24 percent of hip fracture patients age 50 and over die in the year following the fracture.
• Every year, of nearly 300,000 hip fracture patients, one-quarter end up in nursing homes and half never regain previous function.
Osteoporosis is costly.
• Osteoporosis-related bone breaks cost patients, their families and the healthcare system
• By 2025, experts predict that osteoporosis will be responsible for three million fractures resulting in $25.3 billion in costs.
Osteoporosis is preventable.
• About 85-90 percent of adult bone mass is acquired by age 18 in girls and 20 in boys. NOF is currently updating a scientific manuscript regarding Peak Bone Mass and how people can build and maintain strong bones throughout their lifespan.
• Building strong bones during childhood and adolescence can help prevent osteoporosis later in life.
Osteoporosis is manageable.
• Healthy diet and Regular Exercise can help slow or stop the loss of bone mass and help prevent fractures.
• About half of osteoporosis-related repeat fractures can be prevented with appropriate treatment.

INVESTIGSTIONS FOR OSTEOPOROSIS
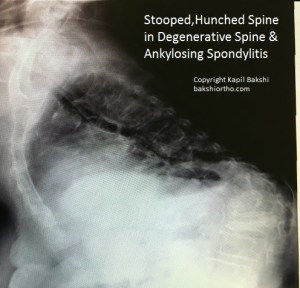
PLAIN X-RAYS
Plain x-rays esp. the wrist, spine and hips give a fair assessment of osteopenia and frank osteoporosis, if noticed, as most physicians mostly lay less importance to this fact.
BLOOD TESTS CONSISTING OF
Basic: Serum Calcium, Phosphorus, Alkaline Phosphatase
TSH and PTH if any abnormal findings for Calcium , Phosphorus and alkaline phosphatase
Advanced: Bone Markers: bone markers can be useful in detecting the imbalance and bone loss.
At least 1 formation marker and 1 resorption marker from the list
List of bone formation markers
- Serum total alkaline phosphatase
- Serum bone–specific alkaline phosphatase
- Serum osteocalcin
- Serum type 1 procollagen (C-terminal/N-terminal): C1NP or P1NP
List of bone resorption markers
- Urinary hydroxyproline
- Urinary total pyridinoline (PYD)
- Urinary free deoxypyridinoline (DPD)
- Urinary collagen type 1 cross-linked N-telopeptide (NTX)
- Urinary or serum collagen type 1 cross-linked C-telopeptide (CTX)
- Bone sialoprotein (BSP)
- Tartrate-resistant acid phosphatase 5b
DEXA* – A bone density test is the best way to diagnose osteoporosis and determine a treatment plan. If your T-score is -2.5 or lower, indicating that you have osteoporosis, or if you have other significant risk factors for breaking a bone, discuss with your doctor about starting an osteoporosis planned tailored treatment plan including medication.
• Discuss the risks and benefits of all medication in the treatment.
• Take recommended amount of calcium and vitamin D daily from foods and/or supplements.
• DEXA should be repeated at least every two years to monitor treatment. After starting a new osteoporosis medicine, many healthcare providers will repeat a bone density test after one year.
*DEXA – Dual-energy X-ray absorptiometry
OSTEOPOROSIS ADVANCED MEDICATIONS OPTIONS AVAILABLE
- FOSAMAX 70 MG
ONCE PER WEEK, for a year and then repeat DEXA SCAN
Mostly very effective, simple and safe, fewer side effects, insurance covered cost effective
2. IBANDRONATE
3 MONTHS – BONVIVA
Prefilled syringes are for single use only. The recommended dose of BONIVA Injection for the treatment of postmenopausal osteoporosis is 3 mg every 3 months administered intravenously over a period of 15 to 30 seconds.
INDICATIVE PRICE 192/-AED approx
4. PROLIA (DENOSUMAB )
ONCE IN 6 MONTHS
60 MG, S/C injection,
INDICATIVE PRICE 1180/- aed approx
5. ZOMETA 1 YEAR
zoledronic acid for inj
Reclast (zoledronic acid) is a bisphosphonate used to treat Paget’s disease, high blood levels of calcium caused by cancer (hypercalcemia of malignancy, multiple myeloma (a type of bone marrow cancer) or cancer that has spread from elsewhere in the body to the bone, to treat or prevent osteoporosis in postmenopausal
INDICATIVE PRICE 866/- AED
6. FORTEO
DAILY TERIPERIIDE Inject FORTEO in the thigh or abdomen once daily with the easy-to-use FORTEO delivery device
INDICATIVE PRICE – NA
Patients taking Actonel showed a bone mineral density (BMD) increase of 2.7%, while those taking the Reclast showed increased BMD of over 4%.
REFERENCES
*courtesy from NOF with due permission and sincere thanks, for all the quotes and links, for wider dissemination of information on Osteoporosis
2. Eur J Rheumatol. 2017 Mar; 4(1): 46–56.
Published online 2016 Dec 30. doi: 10.5152/eurjrheum.2016.048
PMCID: PMC5335887
PMID: 28293453
An overview and management of osteoporosis
Tümay Sözen,1 Lale Özışık,2 and Nursel Çalık Başaran2


 musculoskeletal-ultrasound-course-october-7-8-2016-certificate-kapil-bakshi
musculoskeletal-ultrasound-course-october-7-8-2016-certificate-kapil-bakshi