Rotator Cuff Tendinitis
The rotator cuff is a frequent source of pain in the shoulder. Pain can be the result of:
Tendinitis. The rotator cuff tendons can be inflammed or damaged.
Bursitis. The bursa can become inflamed and swell with more fluid causing pain.
Impingement. When your arm rises to shoulder height, the space between the acromion and rotator cuff decreases. The acromion can rub against (‘impinge’) the tendon and the bursa, causing irritating pain.
Cause: Rotator cuff pain is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball, and tennis are vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as construction or painting are also susceptible.
Minor injury can initiate pain. Sometimes, it occurs with no apparent cause (idiopathic).
The symptoms increase when the problem progresses leading to
Pain at night
Loss of muscle strength and range-of-motion
Difficulty doing activities that place the arm behind the back.
Imaging
X-RAYS: PLAIN X-RAYS DO NOT SHOW THE SOFT TISSUES OF THE SHOULDER LIKE THE ROTATOR CUFF  AND ARE USUALLY NORMAL OR MAY SHOW A SMALL BONE SPUR. A SPECIAL X-RAY CALLED AN “OUTLET VIEW,” SOMETIMES WILL SHOW A SMALL BONE SPUR ON THE FRONT EDGE OF THE ACROMION.
AND ARE USUALLY NORMAL OR MAY SHOW A SMALL BONE SPUR. A SPECIAL X-RAY CALLED AN “OUTLET VIEW,” SOMETIMES WILL SHOW A SMALL BONE SPUR ON THE FRONT EDGE OF THE ACROMION.
MRI and Ultrasound: These studies show good images of soft tissues like the rotator cuff tendons. They can show fluid or inflammation in the bursa and rotator cuff and partial tears of the rotator cuff.
The goal of treatment is to reduce pain and restore function. In planning, the doctor will consider age, activity level, and general health.
Initial treatment is nonsurgical and may take several weeks to months, many patients experience a gradual improvement and return to function.
Rest and activity modification, such as avoiding overhead activities.
NSAIDS can reduce pain and swelling. Consult before self medication.
Physical therapist will initially focus on restoring normal motion to the shoulder. Stretching improves range of motion. Difficulty in reaching behind the back may reveal tightness of the posterior capsule of the shoulder. Specific stretching of the posterior capsule can be very effective in relieving pain under guidance leading to a strengthening program for the rotator cuff muscles.
Steroid injection an effective anti-inflammatory may be helpful if initial treatment did not improve the condition. Injecting it into the bursa beneath the acromion can relieve pain sometimes Ultrasound guidance is required.
Prolotherapy and PRP injections have recently shown to be very effective and safe in select conditions.
Arthroscopy and Open Surgical Procedure may be required in some cases.
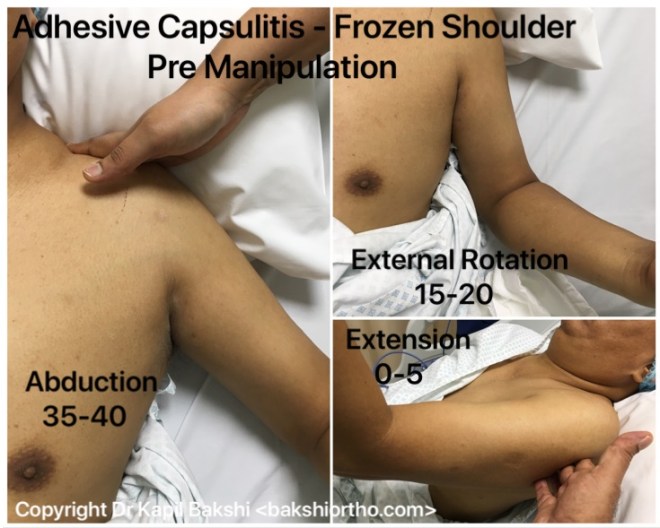
Frozen Shoulder
Adhesive capsulitis, causes pain, loss of motion and stiffness in the shoulder. Over time, the shoulder becomes very hard to move.
Frozen shoulder occurs in about 2% of the general population. It commonly affects people between the ages of 40 and 60, and occurs in women more often than men.
Strong connective tissue, called the shoulder capsule, surrounding the joint thickens and becomes tight, synovial fluid lubricates the shoulder capsule within the joint.
Stiff bands of tissue — called adhesions — develop. In many cases, there is less synovial fluid in the joint.
It develops in three stages:
‘Freezing’ – stage, slowly more and more pain increases and range of motion reduces. Freezing typically lasts from 6 weeks to 6-8 months.
‘Frozen’ – Painful symptoms may in fact improve during this stage, but the stiffness remains. During the 4 to 6 months daily activities may be very difficult.
‘Thawing’ – Shoulder motion slowly improves. Complete return to normal or close to normal strength and motion typically takes from 6 months to 2 years.
Diabetes affecting 10% to 20% of these individuals for unknown reason.
Other diseases like hypothyroidism, hyperthyroidism, Parkinson’s disease, and cardiac disease may potentiate symptoms.
Immobilization for a period of time due to surgery, a fracture, or other injury IA another risk factor reduced by early mobilization on the advice of treating Doctor.
Frozen shoulder generally gets better over time, although it may take up to 2-3 years.
The focus of treatment is to control pain and restore motion and strength through physical therapy.
NSAIDS Non-steroidal anti-inflammatories taken on doctors advice reduce pain and swelling.
Steroid injections is injected directly into the shoulder joint as required.
Physical therapy. Specific exercises will help restore motion under the supervision or via a home program includes stretching and range of motion exercises. Sometimes heat is used to help loosen the shoulder up before the stretching exercises.
Manipulation under Anaesthesia and Arthroscopy are interventional procedures decided in certain cases.