When to see a doctor
Consult if you’re having problems with pain or function of the affected part and you’ve already tried:
Resting your affected part of body
Applying cold or hot to the affected area
Using pain reliving over-the-counter drugs
Disabling joint pain for more than one to two weeks
Excessive swelling or redness in the affected area
Sharp or shooting pain, especially when you exercise or exert yourself
A fever around 38C
Basic Anatomy & Physiology
Tendons are Elastic-cord or rope-like structures that attach from muscle to bone. They glide smoothly through the small tunnel sheath
Age. Middle age (30 to 50, have a higher risk of developing any tenosynovitis than do other age group
Sex. Common in women and in pregnancy
Baby care. Lifting your child repeatedly
Jobs or hobbies that involve repetitive motion
Cold weather, High Humidity worsens the conditions
Complications: Limitations of Range-of-Motion ROM and Stiffness around the joint
Tests for diagnosis.
Imaging helps in the diagnosis, they can help to exclude other causes of your discomfort. Ultrasound or MRI could be used if your bursitis can’t easily be diagnosed by a physical exam alone.
Lab tests. Blood tests (Bone Profile) or an analysis of fluid from the inflamed conditions to pinpoint the cause of inflammation and pain.
Bone Profile includes: CBC (complete blood count), ESR, Serum – Ca, P, Alk PO4, RA Factor test, CRP, UA.
Specific Tests includes: ANA Profile, Anti CCP test, HLA B 27
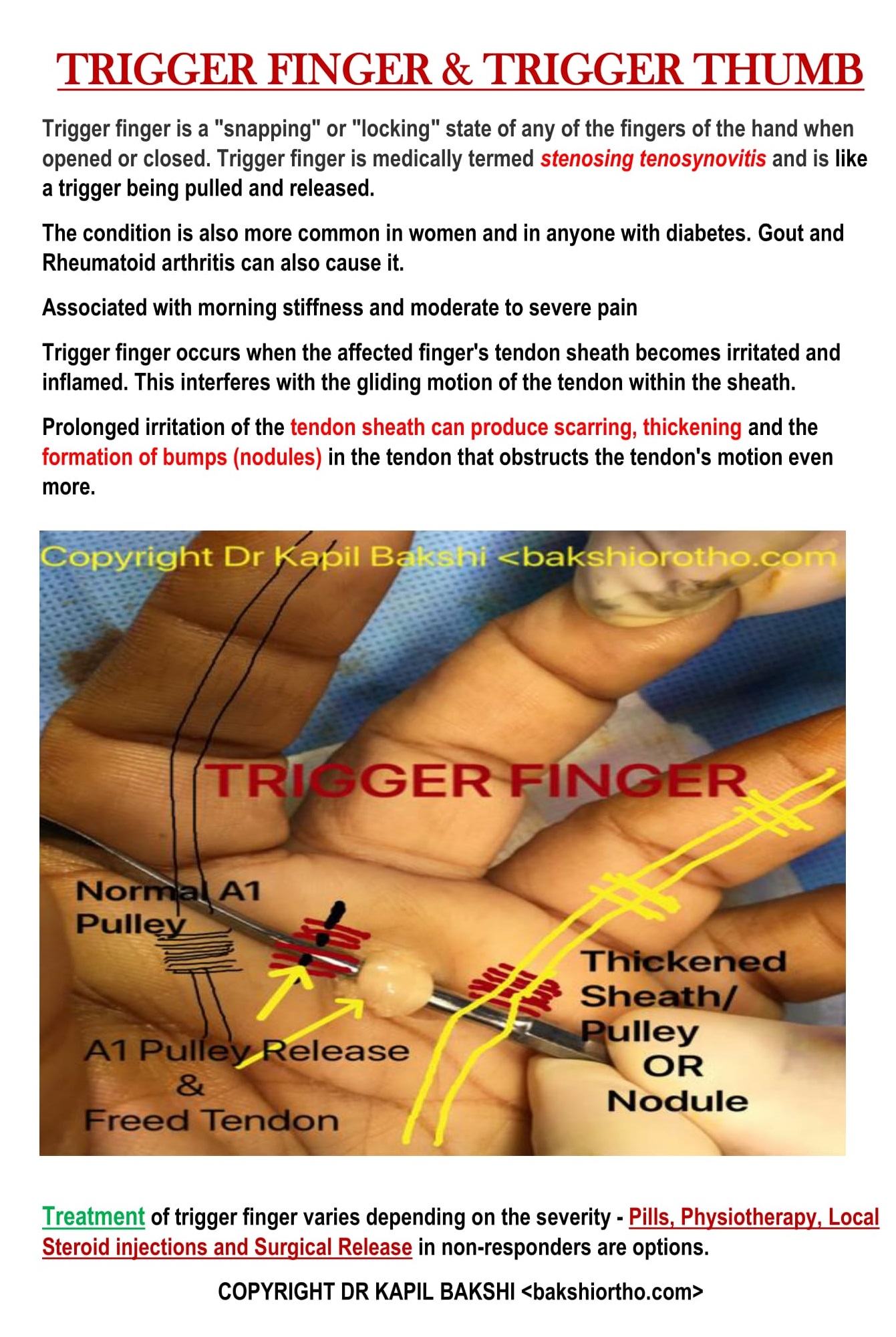
Trigger Fingers “Tennis Finger”
TRIGGER FINGER (1)Trigger finger limits finger movement. When you try to straighten your finger, it will lock or catch before jerking out straight.
Trigger finger is a condition that affects the tendons in your fingers or thumb commonly in index and ring fingers and generally in patients over 45 years of age.
Note a lump or knot in the palm, it may be tender and painful.
Treatment is usually non operative. It usually includes stretching, night splinting,



Bakshi Trigger Pad (patent pending)to keep it warm at night, alternative hot and cold fomentation. Shockwave therapy may be helpful.
Corticicosteriod can have 60 percent success after one injection, may require the 2nd and rarely the third.
Patients with diabetes maybe refractory to treatment. Control of blood sugar closer to normal before injections is desirable.
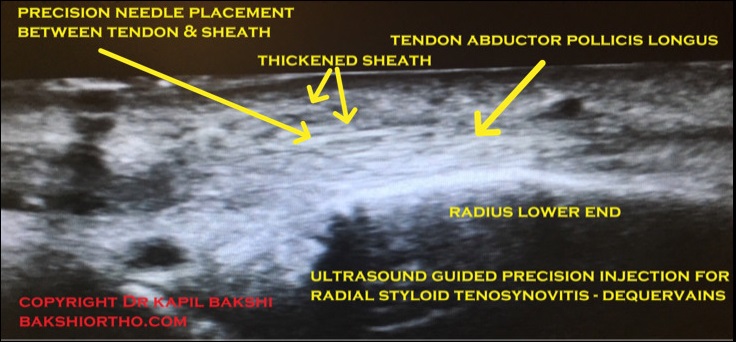
De Quervain’s Tenosynovitis “Tennis Wrist”
It is a painful condition affecting the tendons on the thumb side of your wrist. If you have de Quervain’s tenosynovitis, it will probably hurt when you turn your wrist, grasp anything or make a fist.
Activities that rely on repetitive hand or wrist movement — such as working in the garden, playing racket sports, or lifting your baby — can make it worse.
Symptoms include:

Pain close to the base of the thumb
Swelling around the base of the thumb
Difficulty moving the thumb and wrist on movement
A “sticking” or “stop-go” sensation in thumb when it moves.
Corticosteroid injection helps when physical therapy is not effective. Locally acting steroids are not harmful as these are not water soluble, hence not absorbed in blood stream immediately. Surgical release maybe required.
PLANTAR FASCIITIS OR “TENNIS HEEL”
Plantar fasciitis is one of the most common causes of heel pain. It involves pain and inflammation of a thick band of tissue, called the plantar fascia.
Plantar fasciitis commonly causes pricking or diffuse pain that usually occurs with mornings first step. Once you start walking, after some distance the pain of plantar fasciitis normally decreases, but it may return after long periods of standing or after getting up from a seated position.

Plantar fasciitis is particularly common in people who are overweight and those who wear shoes with inadequate support are at risk. Faulty foot mechanics contribute.
Specific Questions asked
a. Where is the pain
b. Is it always in the same place.
c. Is it worse with the first few steps in the morning.
d. Does it go away with rest.
X-Ray may reveal a calcaneal bony spur. The spur is asymptomatic mostly, the inflammation around it causes pain.
Ultrasound is diagnostic and it shows the quantum of inflammation and the extent of area involved.

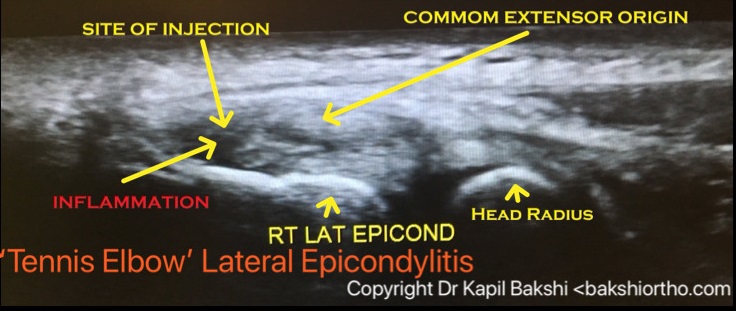
Tennis Elbow ( Lateral Epicondylitis or Epicondylalgia)
It is a painful condition of the elbow caused by overuse and inflammation, playing tennis or other racquet sports can cause this condition. Other sports and activities can flare this and give weak grip strength with inability to lift heavier objects.
Inflammation of the tendons that merge with the forearm muscles on the outer side of the elbow become damaged from repeating the same motions again and again.
Anatomy: Muscles, ligaments, and tendons hold the elbow joint together.
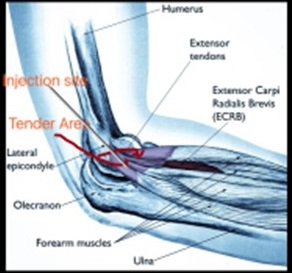
Forearm muscles extend wrist and fingers, forearm tendons – are called extensors – attach the muscles to bone on the lateral epicondyle. The tendon usually involved in tennis elbow is the Extensor Carpi Radialis Brevis (ECRB)
There are many treatment options, old conventional or newer modalities like Prolotherapy with dextrose or PRP (Platelet Rich Plasma)
Physical therapy. Exercises are helpful for strengthening the muscles. Therapist may also perform ultrasonic therapy, ice massage, or muscle-stimulating techniques to improve muscle healing, strength and retard muscle dystrophy.
Brace. Using a brace centered over the back of your forearm may help relieve symptoms by resting the muscles and tendons.
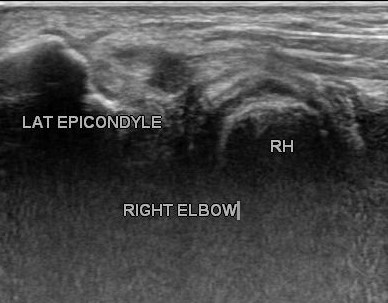
Steroid injections are locally effective anti-inflammatory medicines to relieve symptoms without harm. Corticosteroid injection helps when physical therapy is not effective. Locally acting steroids are not harmful as these are not water soluble, hence not absorbed in blood stream immediately. Ultrasound guidance is used for precision drug delivery to the center of inflammation or to the area of interstitial tear of tendon or partial traumatic tear as shown.



Surgical Treatment
If symptoms do not respond after 6 to 9 months of non-surgical treatments, surgery may be recommended. Excision of proximal portion of annular ligament, release of entire extensor origin, excision of adventitious bursa (if present), resection of hypertrophic synovium. A limited approach consists of excision of diseased Extensor Carpi Radialis Brevis ECRB, resection of degenerative tissue and direct repair to bone. .
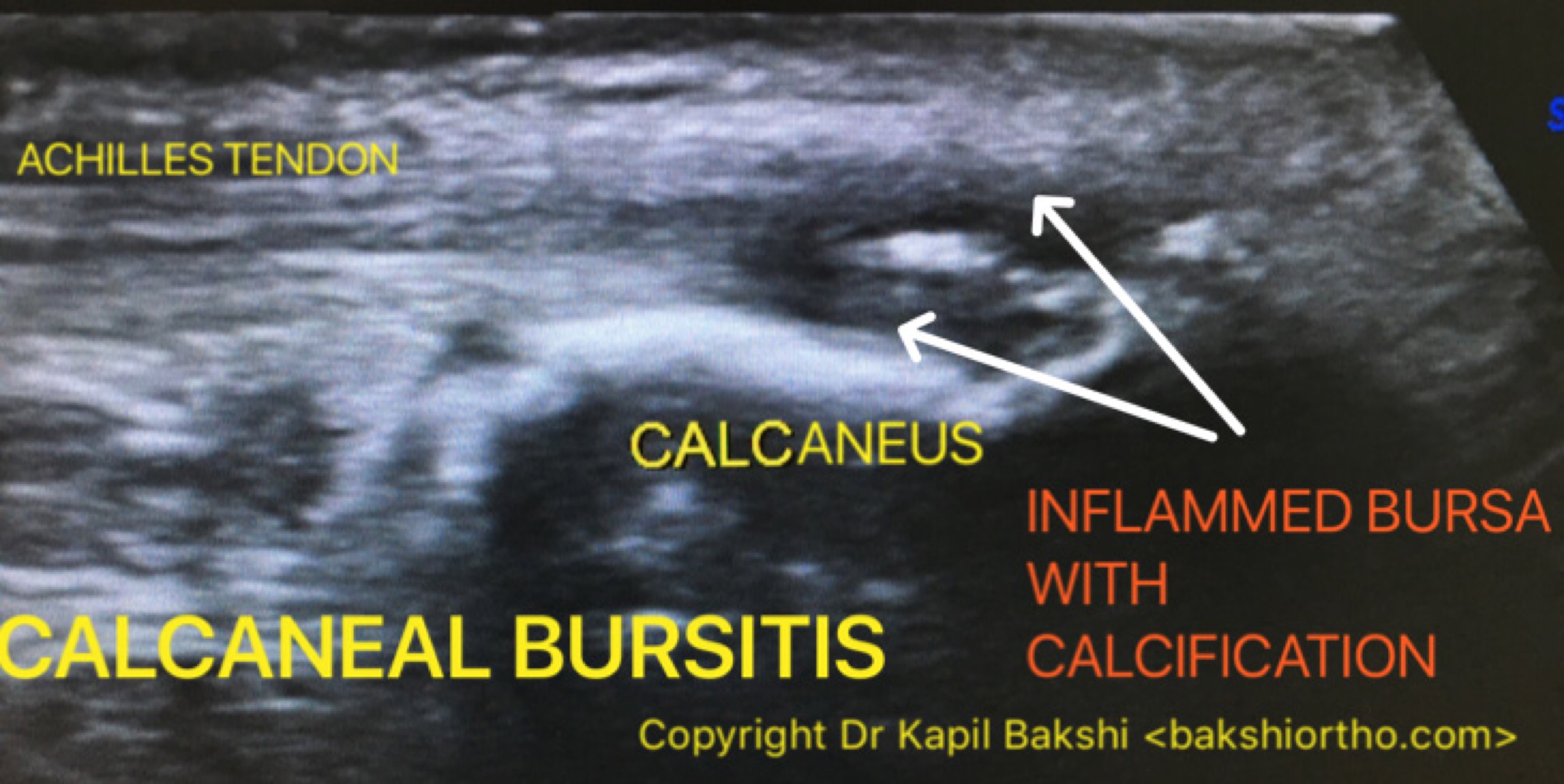
Bursitis Trocanteric, Calcaneal Bursopathy (Heel Pain), Sub-Acromial Impingement Syndrome
Bursitis is a painful condition that affects the small, fluid-filled sacs — called bursae that cushion the bones, tendons and muscles near your joints. Bursitis occurs when bursae become inflamed mostly with swelling and redness.



The most common locations for bursitis are in the shoulder, hip, elbow, knee and Achilles area.
Ultrasound is diagnostic of Calcaneal Bursopathy (Heel pain) and it also depicts early intra-bursal calcification not seen on X-Ray.
Bursitis often occurs near joints that have repetitive motion, other risk factors are Rheumatoid Arthritis, Gout and Diabetes.
Treatment involves rest to the affected joint and protection from further trauma. Bursal pain goes away within few weeks of treatment generally, but recurrent flare-ups are common.
Injection of a corticosteroid into bursa can relieve the pain and inflammation of bursitis. In some cases, ultrasound is used to guide the injection into the affected bursa.
Rotator Cuff Tendinitis
The rotator cuff is a frequent source of pain in the shoulder. Pain can be the result of:
Tendinitis. The rotator cuff tendons can be inflammed or damaged.
Bursitis. The bursa can become inflamed and swell with more fluid causing pain.
Impingement. When your arm rises to shoulder height, the space between the acromion and rotator cuff decreases. The acromion can rub against (‘impinge’) the tendon and the bursa, causing irritating pain.
Cause: Rotator cuff pain is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball, and tennis are vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as construction or painting are also susceptible.
Minor injury can initiate pain. Sometimes, it occurs with no apparent cause (idiopathic).
The symptoms increase when the problem progresses leading to
Pain at night
Loss of muscle strength and range-of-motion
Difficulty doing activities that place the arm behind the back.
Imaging
X-Rays: Plain x-rays do not show the soft tissues of the shoulder like the rotator cuff  and are usually normal or may show a small bone spur. A special X-Ray called an “outlet view,” sometimes will show a small bone spur on the front edge of the acromion.
and are usually normal or may show a small bone spur. A special X-Ray called an “outlet view,” sometimes will show a small bone spur on the front edge of the acromion.
MRI and Ultrasound: These studies show good images of soft tissues like the rotator cuff tendons. They can show fluid or inflammation in the bursa and rotator cuff and partial tears of the rotator cuff.
The goal of treatment is to reduce pain and restore function. In planning, the doctor will consider age, activity level, and general health.
Initial treatment is nonsurgical and may take several weeks to months, many patients experience a gradual improvement and return to function.
Rest and activity modification, such as avoiding overhead activities.
NSAIDS can reduce pain and swelling. Consult before self medication.
Physical therapist will initially focus on restoring normal motion to the shoulder. Stretching improves range of motion. Difficulty in reaching behind the back may reveal tightness of the posterior capsule of the shoulder. Specific stretching of the posterior capsule can be very effective in relieving pain under guidance leading to a strengthening program for the rotator cuff muscles.
Steroid injection an effective anti-inflammatory may be helpful if initial treatment did not improve the condition. Injecting it into the bursa beneath the acromion can relieve pain sometimes Ultrasound guidance is required.
Prolotherapy and PRP injections have recently shown to be very effective and safe in select conditions.
Arthroscopy and Open Surgical Procedure may be required in some cases.
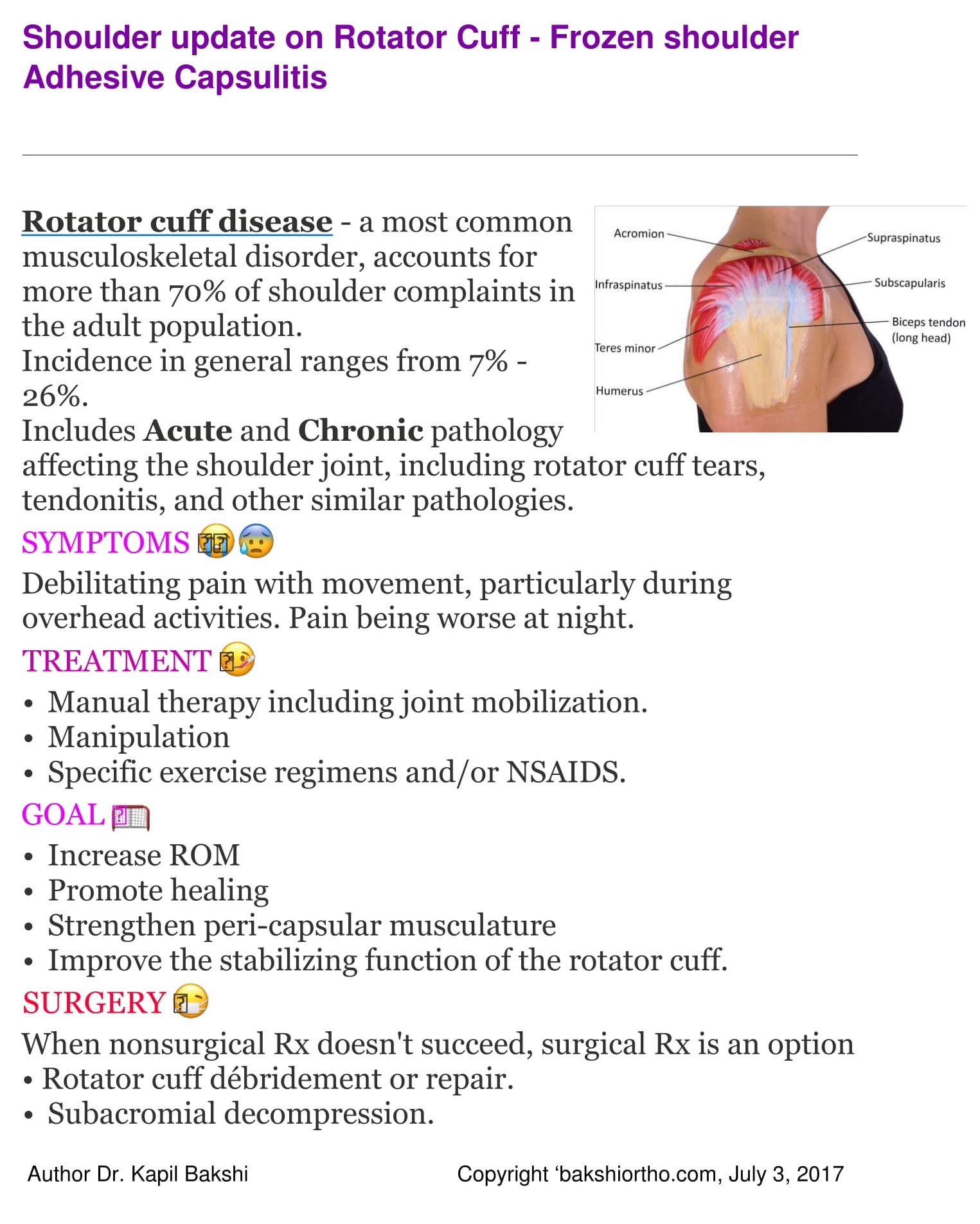
Frozen Shoulder
Adhesive capsulitis, causes pain, loss of motion and stiffness in the shoulder. Over time, the shoulder becomes very hard to move.
Frozen shoulder occurs in about 2% of the general population. It commonly affects people between the ages of 40 and 60, and occurs in women more often than men.
Strong connective tissue, called the shoulder capsule, surrounding the joint thickens and becomes tight, synovial fluid lubricates the shoulder capsule within the joint.
Stiff bands of tissue — called adhesions — develop. In many cases, there is less synovial fluid in the joint.
It develops in three stages:
‘Freezing’ – stage, slowly more and more pain increases and range of motion reduces. Freezing typically lasts from 6 weeks to 6-8 months.
‘Frozen’ – Painful symptoms may in fact improve during this stage, but the stiffness remains. During the 4 to 6 months daily activities may be very difficult.
‘Thawing’ – Shoulder motion slowly improves. Complete return to normal or close to normal strength and motion typically takes from 6 months to 2 years.
Diabetes affecting 10% to 20% of these individuals for unknown reason.
Other diseases like hypothyroidism, hyperthyroidism, Parkinson’s disease, and cardiac disease may potentiate symptoms.
Immobilization for a period of time due to surgery, a fracture, or other injury IA another risk factor reduced by early mobilization on the advice of treating Doctor.
Frozen shoulder generally gets better over time, although it may take up to 2-3 years.
The focus of treatment is to control pain and restore motion and strength through physical therapy.
NSAIDS Non-steroidal anti-inflammatories taken on doctors advice reduce pain and swelling.
Steroid injections is injected directly into the shoulder joint as required.
Physical therapy. Specific exercises will help restore motion under the supervision or via a home program includes stretching and range of motion exercises. Sometimes heat is used to help loosen the shoulder up before the stretching exercises.
Manipulation under Anaesthesia and Arthroscopy are interventional procedures decided in certain cases.