
 Dr Kapil Bakshi has completed the ‘MSK Ultrasound Course and Hands on training’ from the worlds premier Radiology & Ultrasound training institute at Thomas Jefferson University Hospital, Philadelphia this October, 2016 to refine and update current knowledge and technology used. Several lectures on the basics of MSK ultrasound for other practitioners given.
Dr Kapil Bakshi has completed the ‘MSK Ultrasound Course and Hands on training’ from the worlds premier Radiology & Ultrasound training institute at Thomas Jefferson University Hospital, Philadelphia this October, 2016 to refine and update current knowledge and technology used. Several lectures on the basics of MSK ultrasound for other practitioners given.
Dr. Bakshi is one of the few Orthopedic Surgeons who do their own Ultrasound for the diagnosis, while treating the pathology with precision latest high (MHz) frequency ultrasound guided Local and Intra-articular injections and Regenerative Therapies in sterile operative conditions. The new probe scans with clarity close to an MRI, serving as an as an “Instant Hand-held Dynamic MRI”
MSK ultrasound is low cost, saves time as it is done as an office procedure, many times the pathology is so apparent that an MRI is often saved, saving further costs of treatment to the insurance companies and cash paying patients.
Ultrasound is safe and has no ionizing radiation.
Further the scan is done for the area of interest according to the clinical findings seen and felt by the treating surgeon, these are then visualized by the ultrasound. Unwanted scanning of normal areas is not done saving time both for the patient and the doctor. The few radiologists who have the skills of doing soft tissue MSK ultrasound scan the entire area as they are not aware of where the pathology is.
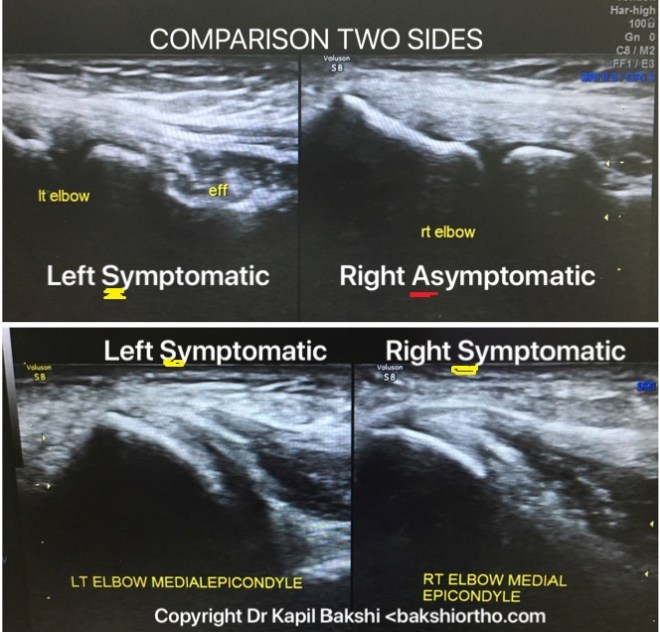
Comparison of two sides can be done
Advantage over plain X-Ray
There are times when the hairline and other smaller fractures cannot be easily diagnosed over overlapping bones, clinically the patient has swelling and is tender locally, Ultrasound is helpful in establishing the diagnosis


Advantage over MRI
a. Dynamic ‘Real time ultrasound and interventions’– motion of joint, muscle and tendon is evaluated ‘live’ with the ultrasound with the ensuing motion.
b.Stress test evaluation of ligament injuries.
c. Floating debris and non opaque foreign bodies in an effusion.
d. Contra-lateral side used for comparison.
In a short span of time we will introduce ultrasound guided percutaneous surgery with a 2-3 mm incision using micro endoscopic surgical knife and ultrasound guided Hypodermic needle surgeries under local anesthetic as an office procedure.
Indications of MSK Ultrasound
Pathologies of
1. Tendon – Tendinosis, Tendinitis, Tendon Rupture and Tears, Strains,Tenosynovitis, Tendon Subluxations and Dislocations.
2. Muscle- Sporting injuries-Tears and Strains, Myositis, Hernia, Masses, Cysts.
3. Joints – Synovial thickening and Effusion, Avulsion Fractures
4. Cartilage – Ulcers and Erosion, thinning and Calcification.
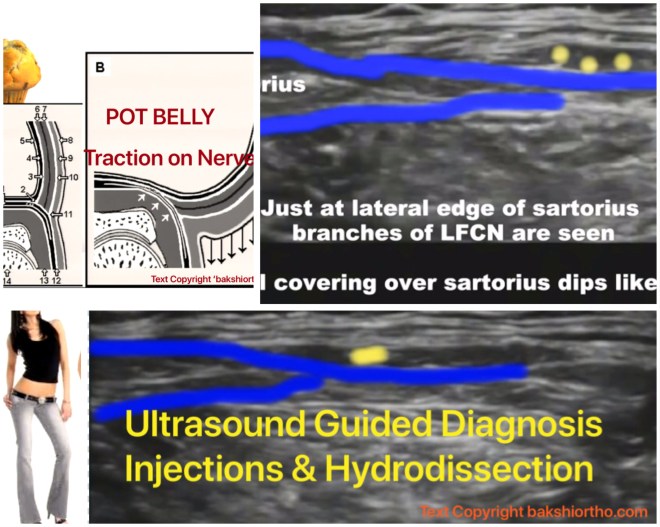
5. Nerve – Entrapment, Injury, Hematoma around it, Neurofibroma
6. Ligaments – Tears and Strains.
7. Bones – esp Ribs Fracture not seen on plain film, Stress fractures
8. Foreign bodies – Fish bone, Wood splinters, Tooth picks.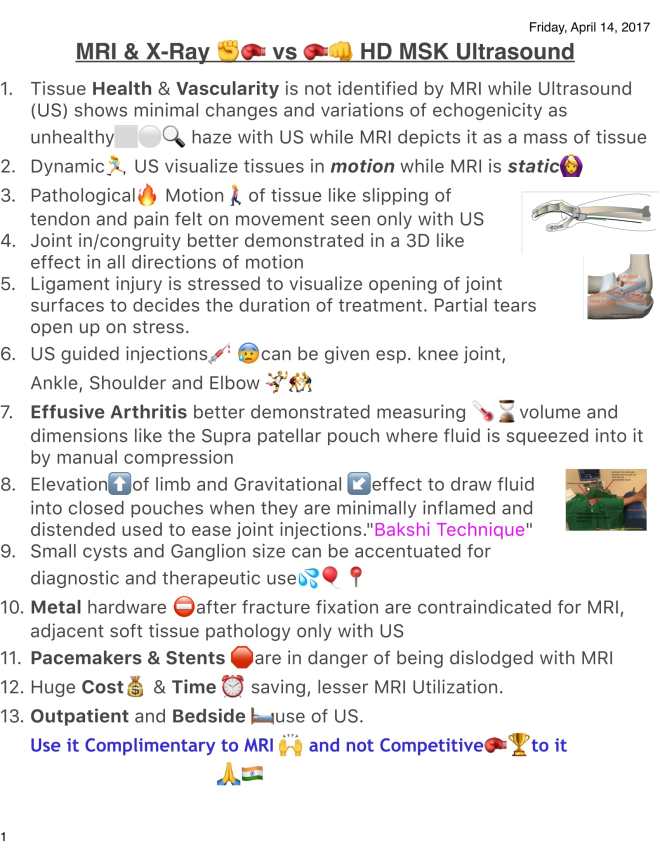
‘Bakshi Technique’ of Intra-Articular Ultrasound Guided Knee Injections
Elevate the limb on a roll under the leg, extend the knee to the maximum and relax the patient.
3% xylocaine is used for local anesthetic to inject around the suprapatellar pouch from the skin inwards. Use a 18 gauge canula with needle to enter Suprapatellar Pouch under Ultrasound image guidance under sterile conditions using the aseptic technique and sterile ultrasound gel.
Test whether you are inside the cavity by injecting a few drops of leftover xylocaine in the syringe. Inject ‘Lubricant'(Viscosupplement) or PRP.
Save images for documentation.

msk-ultrasound-course-certificatemusculoskeletal-ultrasound-course-october-7-8-2016-certificate-kapil-bakshimusculoskeletal-ultrasound-course-october-7-8-2016-certificate-kapil-bakshi
Kapil Bakshi CME Jefferson 2021
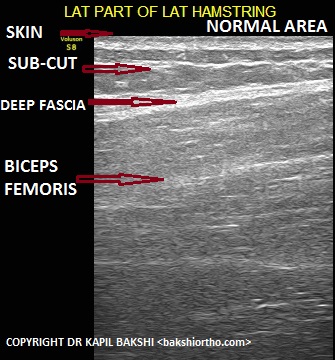
Ultrasound of Normal Tendon, Muscle, Nerve, Cartilage
Muscle
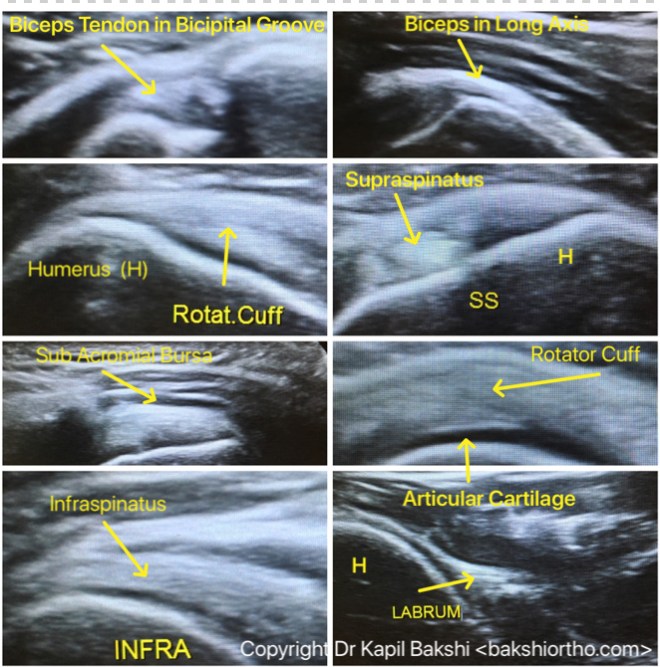
SHOULDER ULTRASOUND
Examination, Procedure and Positioning
The long head of the biceps tendon – forearm in supination and resting on the thigh or with the arm in slight external rotation. The tendon is examined in a transverse plane (short axis), where it emerges from under the acromion, to the musculo-tendinous junction.
Subscapularis tendon, the elbow remains at the side while the arm is placed in external rotation. The subscapularis is imaged from the musculo-tendinous junction to the insertion on the lesser tuberosity. Dynamic evaluation – patient moves from internal to external rotation.
Supraspinatus tendon, the arm can be extended posteriorly, and the palmar aspect of the hand can be placed against the superior aspect of the iliac wing with the elbow flexed and directed toward the mid line (instruct the patient to place the hand in the back pocket. Transducer
Posterior aspect of the infraspinatus and teres minor tendons should be examined by placing the transducer at the level of the glenohumeral joint below the scapular spine while the forearm rests on the thigh with the hand supinated. Internal and external rotation. Visualize the teres minor tendon, the medial edge of the probe should be angled slightly inferiorly.
Rotator cuff, the cuff should be compressed with the transducer to detect non-retracted tears. Contralateral side evaluation useful. Dynamic evaluation – assess the cuff tear extent. In patients with a rotator cuff tear, the supraspinatus, infraspinatus, and teres minor – examined for atrophy.
Normal Shoulder Sonogram

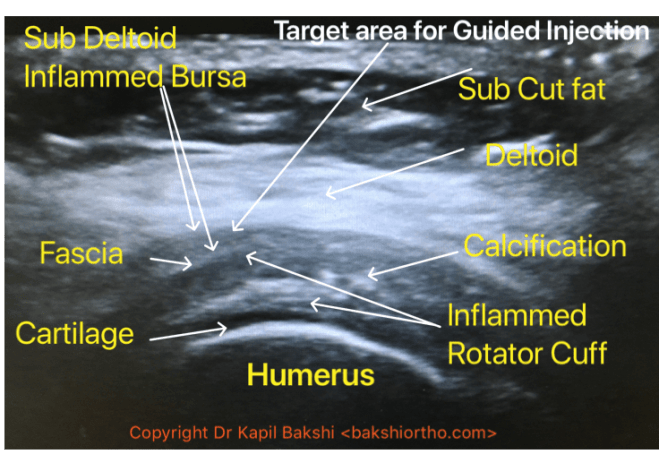
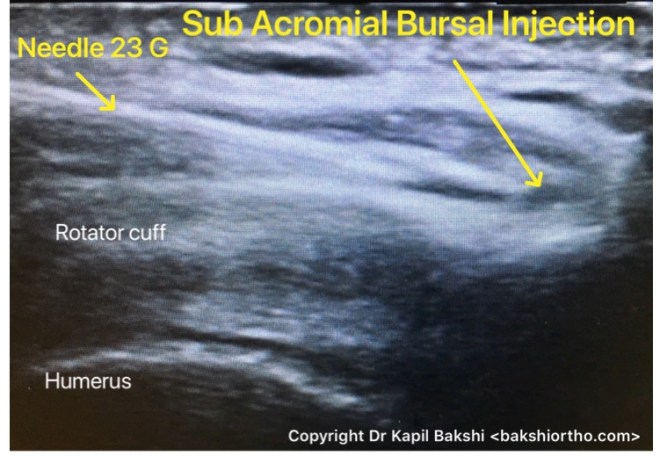

Subacromial-subdeltoid – bursal thickening or fluid.
Glenohumeral joint with the probe placed in the transverse plane from a posterior approach to evaluate for effusions, intra-articular loose bodies, synovitis, or bony abnormalities. Supra scapular notch and spinoglenoid notch also may be evaluated.
Acromioclavicular joint should be evaluated with the probe placed at the apex of the shoulder, bridging the acromion and distal clavicle.
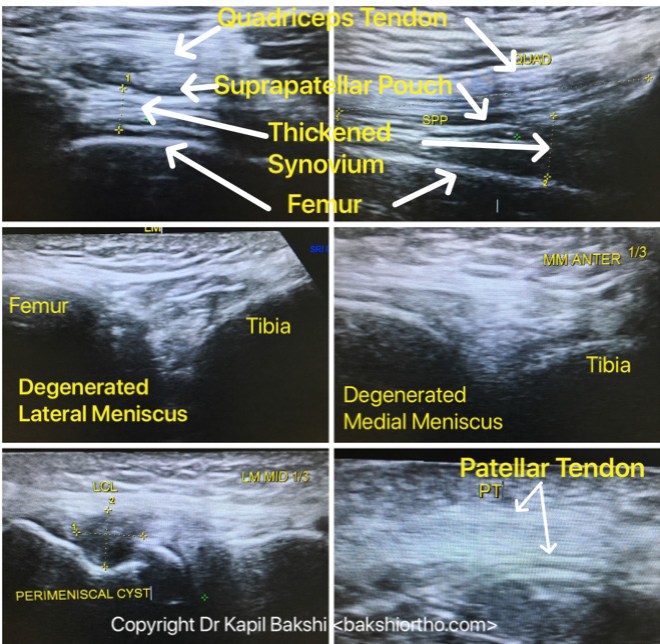
KNEE ULTRASOUND
Pathologies visualized on Ultrasound are Synovitis, Effusion in Suprapatellar Pouch, Disorders of Retinaculum, Meniscus Degenerative and Traumatic Tears, Quadriceps and Patellar Tendinitis and Tendinosis, Baker’s Cysts, Meniscal Cysts and Ganglion.
Hemarthrosis and Synovitis with Effusion


Causes of Chondromalacia patella:
* Anatomical or Mechanical Variations: Q-angle: The most important cause of Chondromalacia patella is abnormal Q-angle. Normal Q-angle for men is 14◦ and for women, it is 17◦. The lateral pull of the patella is increased if this angle is increased which then can lead to Chondromalacia patella.
* Muscle tightness: If the rectus femoris muscle is stiff due to spasm, it affects the patellar movement when the knee is bent. Iliotibial band muscle tightness with tight lateral retinaculum pulls the patella to the lateral side of the knee when the knee is bent.
* Trauma: Knee instability caused by a previous cruciate ligament or meniscal deficiency, trauma or misuse of the knee can lead to Chondromalacia patella. Repetitive trauma and inflammatory conditions like arthritis can increase the incidence of chondromalacia.
‘Chondromalacia
* grade I : *
arthroscopically: softening or swelling of cartilage
* grade II
*arthroscopically: blister-like swelling within soft areas of articular cartilage
* grade III
* arthroscopically: partial thickness cartilage loss with fibrillation (crab-meat appearance)
* grade IV
*arthroscopically: full thickness cartilage loss, erosions and bone-on-bone in more than 50 % surface areas. There are with underlying bone reactive changes with cortical defects,cartilage destruction with exposed subchondral bone

Meniscal Tears and Bursa under Medial Collateral Ligament



Meniscal Cyst as seen on Ultrasound and MRI Comparison




 Patellar Tendinitis
Patellar Tendinitis
This is an inflammatory condition, in acute stages it is associated with pain, swelling and localized tenderness. The skin could be red and warm to touch.
The x-rays are generally normal but Ultrasound can clearly demonstrate the quantum of inflammation, seen closer to tibial tuberosity and patellar ends as in this case.
Lateral Collateral Ligament Injury





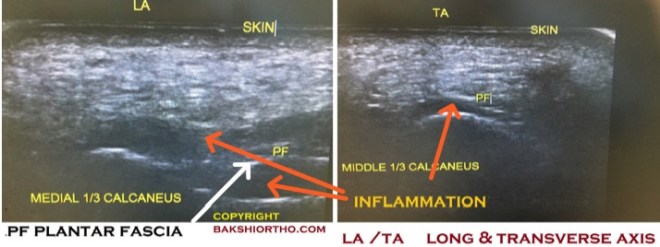
ANKLE AND HEEL ULTRASOUND


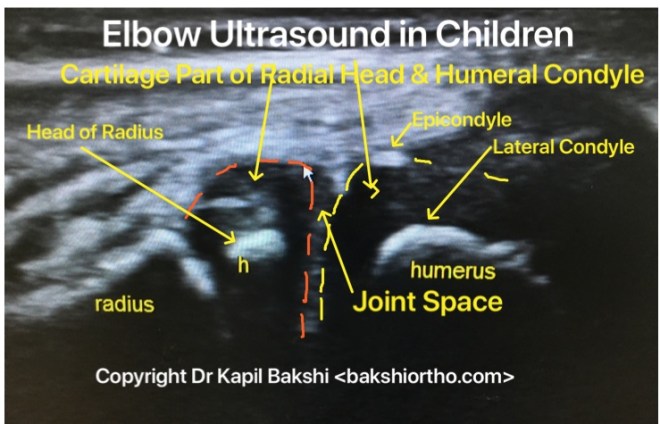
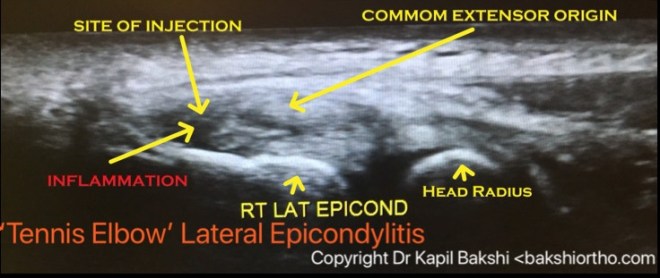
ELBOW ULTRASOUND




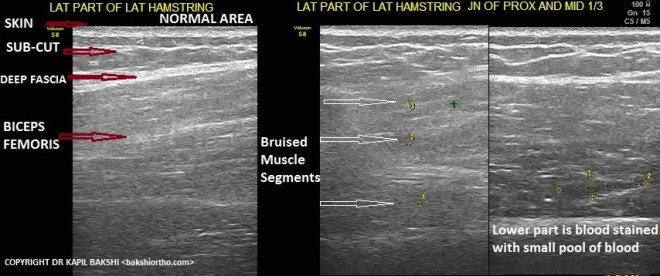
Muscle trauma and Bruising

Carpal Tunnel Compression Syndrome

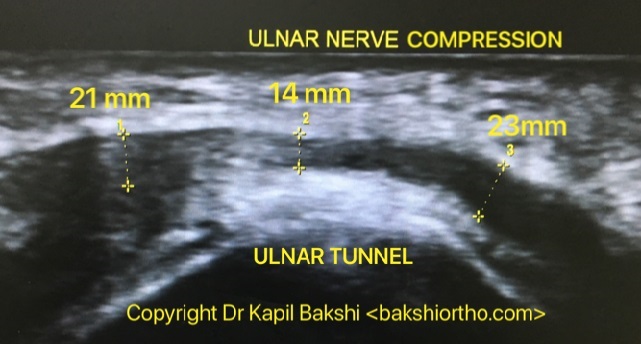
Ulnar Tunnel Compression at Elbow
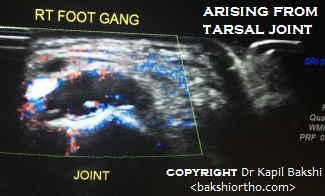
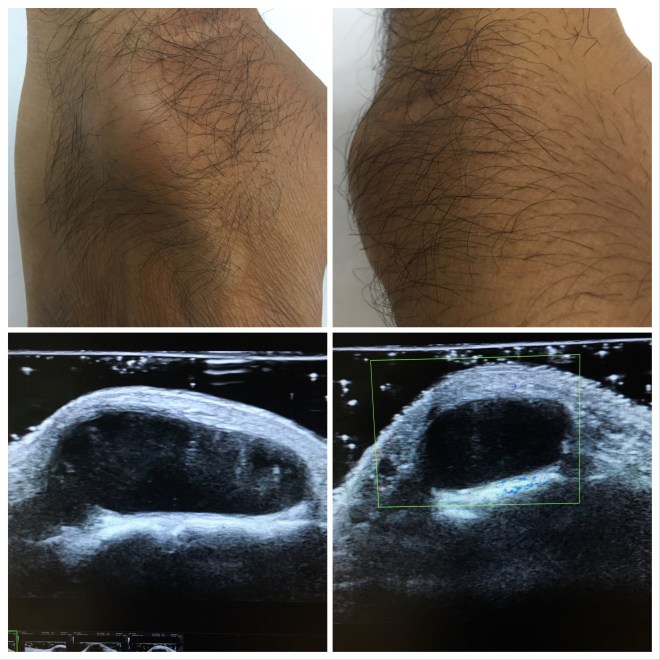
Ganglion

Ganglion Dorsum of Hand

Trigger Thumb

SMALL JOINTS
1ST METATARSOPHALYNGEAL JOINT

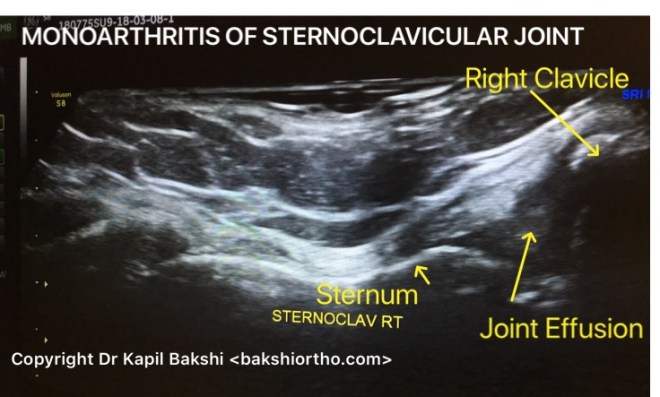
STERNOCLAVICULAR JOINT

Implant Location
Implant location without X-rays, infection, fluids collection in a bursa or pus collection and loosening can be visualized. Metal Foreign Body Detection can be done and extraction made easier with 2-plane injection needle technique.
Implant on Xray and Ultrasound
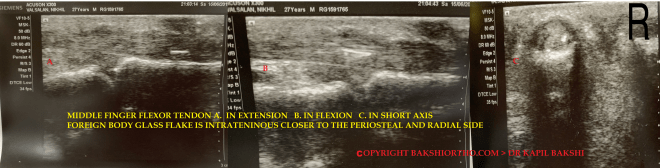
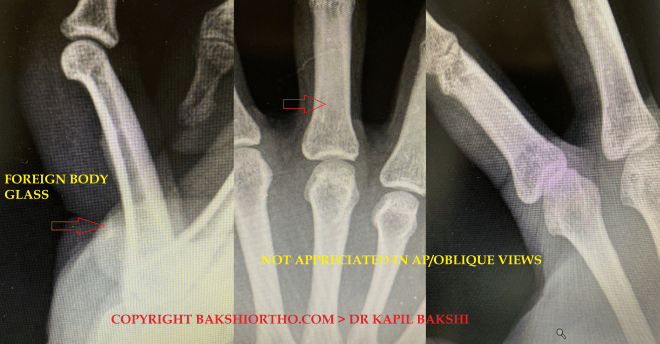
Foreign body visualization
Ultrasound can scan various foreign bodies like metal, glass and wood
Summary
MSK ultrasound is low cost, saves time as it is done as an office procedure, many times the pathology is so apparent that an MRI is often saved, saving further costs of treatment to the insurance companies and cash paying patients.
Ultrasound is safe and has no ionizing radiation.
Further the scan is done for the area of interest according to the clinical findings seen and felt by the treating surgeon, these are then visualized by the ultrasound. Unwanted scanning of normal areas is not done saving time both for the patient and the doctor.
Presentation at AAOS, American Academy of Orthopedic Surgeons, Las Vegas, USA March 2019
Abstract P0248, Category Practice Management – accepted and slated for presentation at the conference.
“Musculoskeletal Ultrasound – Unveiling its Vast Potential to Popularize it in Medically Developing Countries in Contrast to MRI for Mass Diagnostic Use and Guided Procedures”

A concept for the mass use of cheaper MSK ultrasound for guided Procedures and precision placement of drug at the target site maximizing the efficiency and effectiveness.

Presentation at SICOT 39th World congress of Orthopedics, Montreal, Canada, 10-13 Oct 2018
MSK Ultrasound – Grading of Chondromalacia Knee (Certificate attached)
A single frame 2 Pole Ultrasound in 2 minute to diagnose and guide treatment of Chondromalacia in knees, one of the most common cause of knee pain reaching near epidemic proportions due to lack of exercise, weak quadriceps and early aging of knees
Click to access Abstract-Book-Posters.pdf
SCROLL to 50585 abstract

A patient asked “Is the Ultrasound causing radiation effects.”
Answer: No, these are sound waves. Just as Shouting near and to the body part will damage
Good morning sir
Do u offer any online or offline fellowship for MSK Ultrasound?
Not yet, but if people like you encourage me I can think on that lines. Paucity of time is the issue. I have about 7 years of ultrasound experience and presentation in AAOS and SICOT on ultrasound.